Given the importance of NHM in providing affordable healthcare to a large section of the populace, different data/information about the scheme should be readily available and accessible to the common masses. Figure 11 lists essential NHM data points/information that are useful to various stakeholders for Durg. Hence, their availability and accessibility would be useful. The current level of information available has been evaluated as under:
Transparency and Accountability Index
Availability of Information and Comprehensiveness
Information on funds available
Yes
Information on funds utilized
Yes
Information on eligible beneficiaries under various sub-components of NHM
Yes
Gender-wise disaggregation of beneficiary data
No
Caste-wise disaggregation of beneficiary data
No
Geographical granularity of the fiscal indicator
Fund availability: Available Block-wise and component-wise
Expenditure of funds: Available only Block/PHC-wise and not component-wise
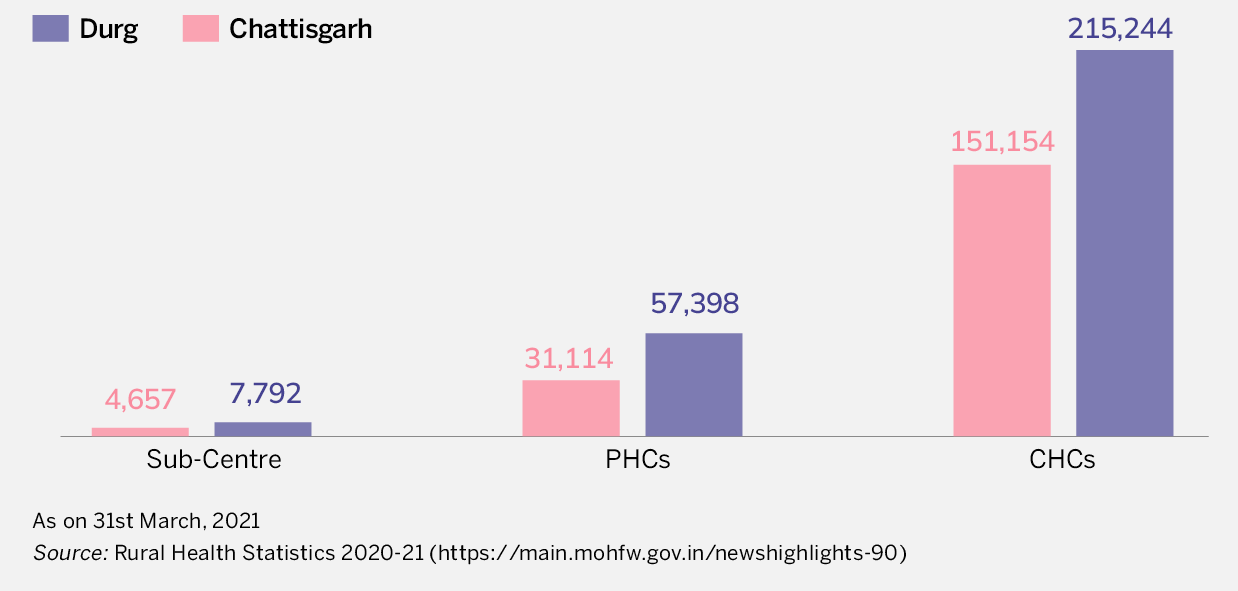
Information on number of PHCs/DH/SDH
Yes
Accessibility
Language in which information is available
English only
Compatibility on devices
Phone, tablet, laptop friendly
Timeliness
How frequently is data updated?
Yearly
Relevance
How relevant would users find it?
(i) Fiscal information pertaining to the budget approved/allocated is extensively available in state/district PIPs and RoPs for various years by components, but it is not aligned with the geographical granularity of the district. Expenditure data for various years is available only by geography and component, making it difficult to arrive at an aggregate picture of health sector spending in the district.
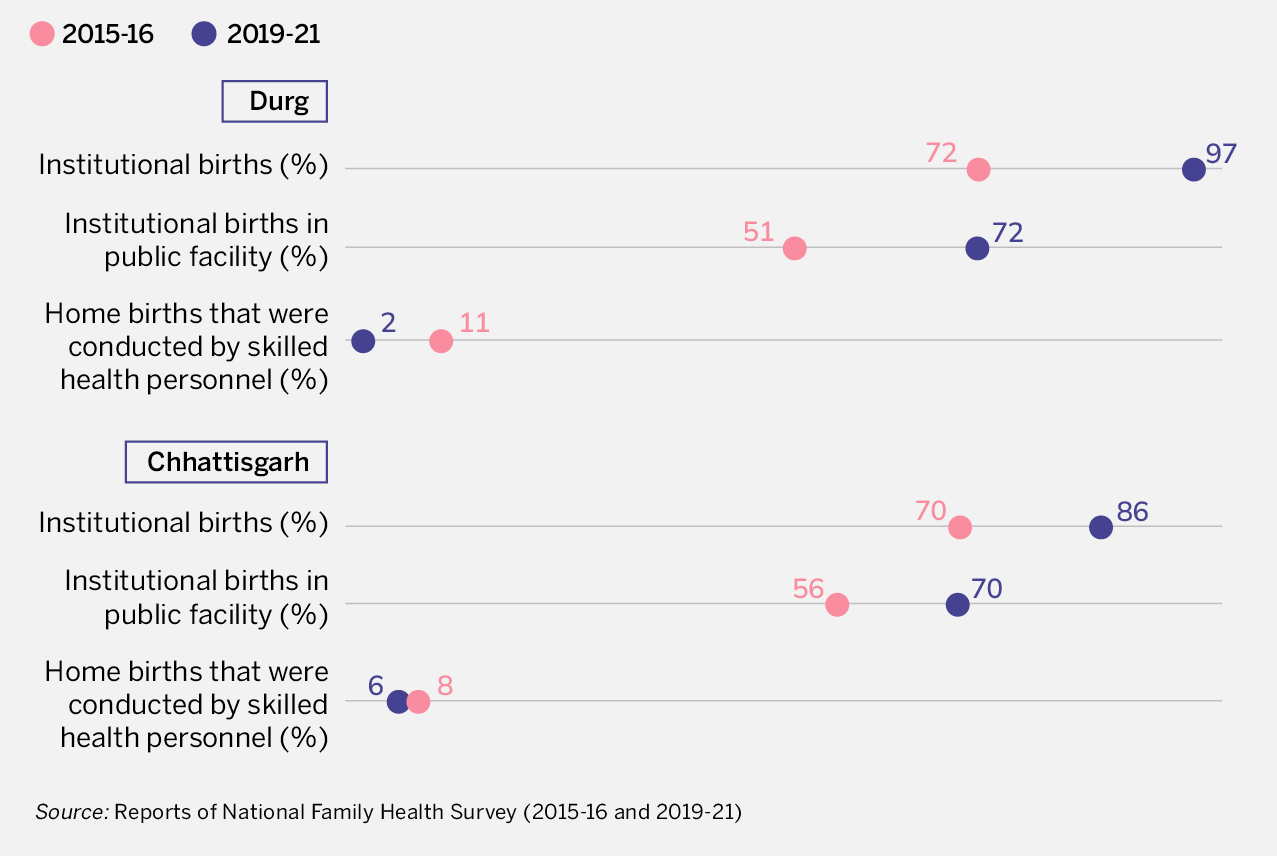
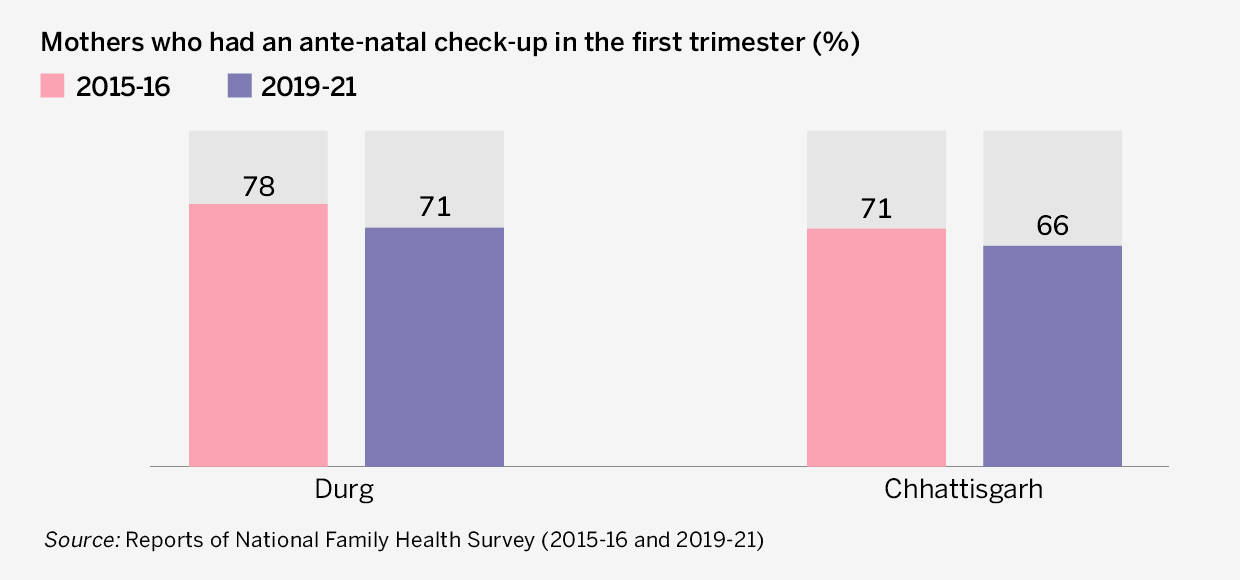
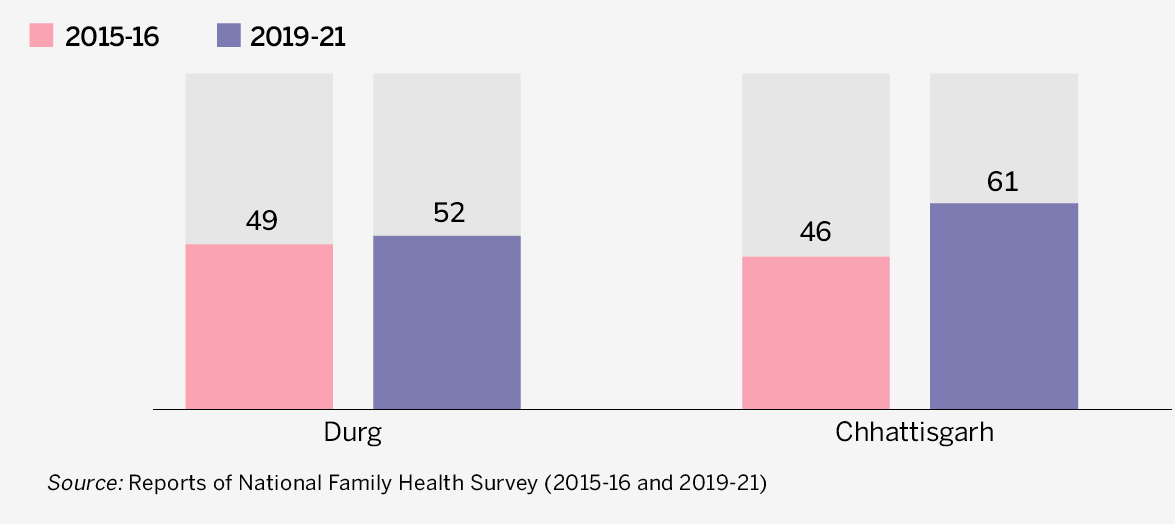
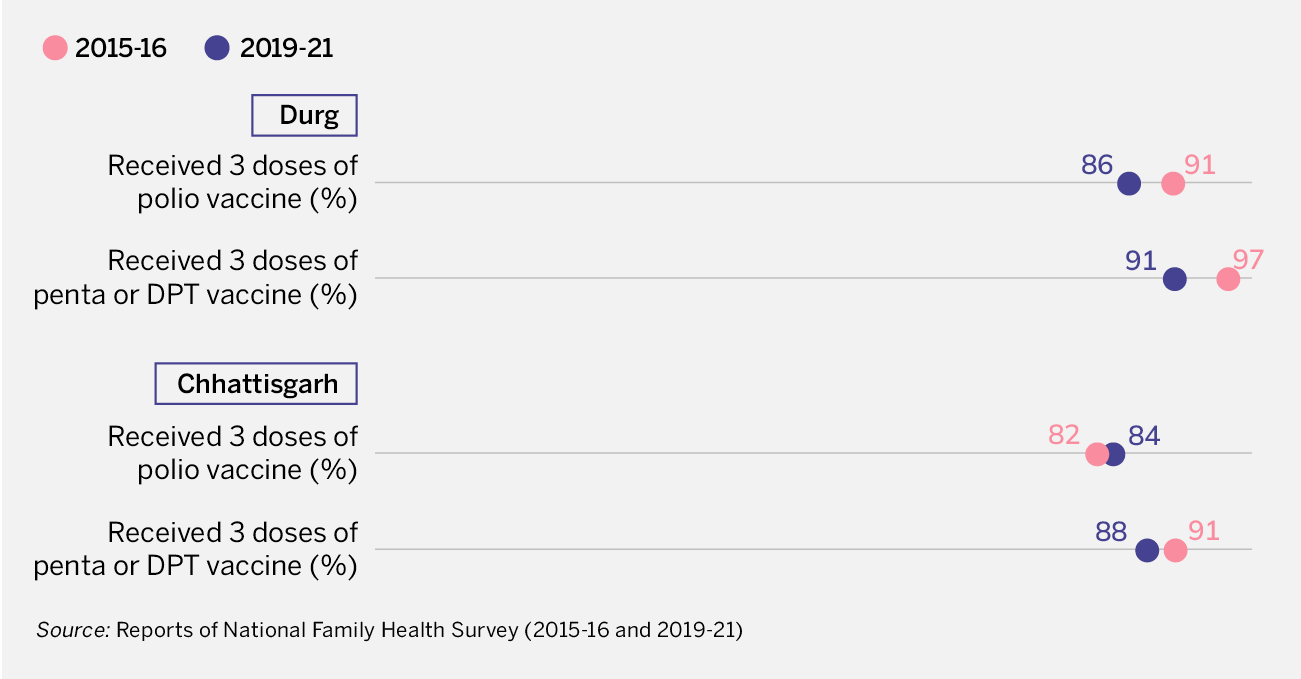
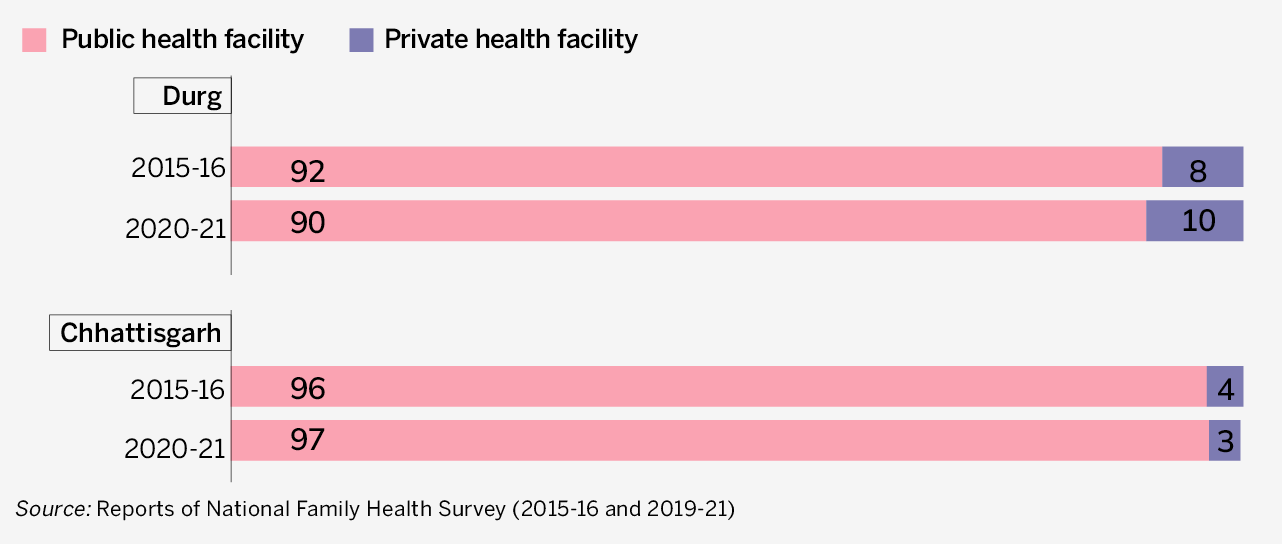
(ii) Data sources pertaining to various health outcomes, such as NFHS and HMIS, are quite extensive in their coverage and in providing adequate information in the public domain.
Reliability
Is the data reliable?
Relevant audit reports are not available on the NHM website. Hence, reliability of data has remained an issue.
Accountability and Citizens' Participation
Availability of information on social audit
Provisions for the same are not available on the NHM website.
Availability of information on grievance redressal
Provisions for the same are not available on the NHM website.